Overview
Although
tibial plateau fracture was originally termed a bumper or fender
fracture, only 25% of tibial plateau fractures result from impact with
automobile bumpers. The most common mechanism of injury involves axial
loading, such as results from a fall. Other patterns of injury result
from laterally directed forces or from a twisting injury. In all cases,
force is directed from the femoral condyles onto the medial and lateral
portions of the tibial plateau, resulting in fracture. In younger
patients, the most common pattern of fracture is splitting, while in
older, more osteoporotic patients, depression fractures typically are
sustained.
Examples of tibial plateau fractures are provided in the images below:
 Tibial
plateau fractures. Line drawings of Schatzker types I, II, and III
tibial plateau fractures. Type I consists of a wedge fracture of the
lateral tibial plateau, produced by low-force injuries. Type II combines
the wedge fracture of the lateral plateau with depression of the
lateral plateau. Type III fractures are classified as those with
depression of the lateral plateau but no associated wedge fracture.
Tibial
plateau fractures. Line drawings of Schatzker types I, II, and III
tibial plateau fractures. Type I consists of a wedge fracture of the
lateral tibial plateau, produced by low-force injuries. Type II combines
the wedge fracture of the lateral plateau with depression of the
lateral plateau. Type III fractures are classified as those with
depression of the lateral plateau but no associated wedge fracture.  Tibial
plateau fractures. Line drawings of Schatzker types IV, V, and VI
tibial plateau fractures. Type IV is similar to type I fracture, except
that it involves the medial tibial plateau as opposed to the lateral
plateau. Greater force is required to produce this type of injury. Type V
fractures are termed bicondylar and demonstrate wedge fractures of both
the medial and lateral tibial plateaus. Finally, type VI fractures
consist of a type V fracture along with a fracture of the underlying
diaphysis and/or metaphysis.
Tibial
plateau fractures. Line drawings of Schatzker types IV, V, and VI
tibial plateau fractures. Type IV is similar to type I fracture, except
that it involves the medial tibial plateau as opposed to the lateral
plateau. Greater force is required to produce this type of injury. Type V
fractures are termed bicondylar and demonstrate wedge fractures of both
the medial and lateral tibial plateaus. Finally, type VI fractures
consist of a type V fracture along with a fracture of the underlying
diaphysis and/or metaphysis. 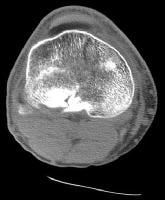 Tibial
plateau fractures. CT image through the tibial plateau shows a fracture
of the posterior aspect of the lateral tibial plateau, which is the
source of the lipohemarthrosis.
Tibial
plateau fractures. CT image through the tibial plateau shows a fracture
of the posterior aspect of the lateral tibial plateau, which is the
source of the lipohemarthrosis.  Tibial
plateau fractures. MRI of the knee in a patient with tibial plateau
fracture and lipohemarthrosis. Three layers of effusion are demonstrated
on this proton density sequence: fat, red blood cells, and serum.
Low-signal intensity in the tibial plateau corresponds to the site of
fracture.
Tibial
plateau fractures. MRI of the knee in a patient with tibial plateau
fracture and lipohemarthrosis. Three layers of effusion are demonstrated
on this proton density sequence: fat, red blood cells, and serum.
Low-signal intensity in the tibial plateau corresponds to the site of
fracture.  Tibial
plateau fractures. Radiograph of the knee shows lateral plateau
splitting, a Schatzker I injury. There is no articular depression. Soft
tissue injuries (eg, to cruciate and collateral ligaments) occur in
approximately 10% of patients. In particular, medial plateau injuries
may result in fracture of the fibular head, which may injure the
peroneal nerve or may be associated with popliteal artery occlusion.
Patients may present with a knee effusion, pain, and joint stiffness.
Finally, although severe fractures often are repaired surgically, both
operatively and nonoperatively treated fractures are at risk of
developing posttraumatic osteoarthritis as a result of ligamentous
injuries with resultant instability as well as articular discongruities,
biomechanical alteration of normal compressive forces, and cartilage
damage.
Tibial
plateau fractures. Radiograph of the knee shows lateral plateau
splitting, a Schatzker I injury. There is no articular depression. Soft
tissue injuries (eg, to cruciate and collateral ligaments) occur in
approximately 10% of patients. In particular, medial plateau injuries
may result in fracture of the fibular head, which may injure the
peroneal nerve or may be associated with popliteal artery occlusion.
Patients may present with a knee effusion, pain, and joint stiffness.
Finally, although severe fractures often are repaired surgically, both
operatively and nonoperatively treated fractures are at risk of
developing posttraumatic osteoarthritis as a result of ligamentous
injuries with resultant instability as well as articular discongruities,
biomechanical alteration of normal compressive forces, and cartilage
damage.
 Tibial
plateau fractures. Cross-table lateral radiograph of the knee shows the
lipohemarthrosis within the suprapatellar bursa. The fracture itself is
not seen well. Tibial
plateau fractures. CT image through the tibial plateau shows a fracture
of the posterior aspect of the lateral tibial plateau, which is the
source of the lipohemarthrosis.
Tibial
plateau fractures. Cross-table lateral radiograph of the knee shows the
lipohemarthrosis within the suprapatellar bursa. The fracture itself is
not seen well. Tibial
plateau fractures. CT image through the tibial plateau shows a fracture
of the posterior aspect of the lateral tibial plateau, which is the
source of the lipohemarthrosis.  Tibial plateau fractures. Axial CT image through the knee shows a layering lipohemarthrosis. Tibial
plateau fractures. MRI of the knee in a patient with tibial plateau
fracture and lipohemarthrosis. Three layers of effusion are demonstrated
on this proton density sequence: fat, red blood cells, and serum.
Low-signal intensity in the tibial plateau corresponds to the site of
fracture. CT is used by most orthopedists to further
characterize fractures of the tibial plateau and assess the depression
of the tibia and the degree of diastasis (splitting) of the fractured
parts to plan for surgical intervention. Generally, slice thickness
should be minimized (1 mm is ideal) and high milliamperage-second (mAs)
technique used.[1, 2, 3]
Tibial plateau fractures. Axial CT image through the knee shows a layering lipohemarthrosis. Tibial
plateau fractures. MRI of the knee in a patient with tibial plateau
fracture and lipohemarthrosis. Three layers of effusion are demonstrated
on this proton density sequence: fat, red blood cells, and serum.
Low-signal intensity in the tibial plateau corresponds to the site of
fracture. CT is used by most orthopedists to further
characterize fractures of the tibial plateau and assess the depression
of the tibia and the degree of diastasis (splitting) of the fractured
parts to plan for surgical intervention. Generally, slice thickness
should be minimized (1 mm is ideal) and high milliamperage-second (mAs)
technique used.[1, 2, 3]
MRI may be used as well for this determination but often is not readily available. MRI is excellent for depicting ligamentous and meniscal injuries.
Arteriography (and possibly MR angiography) may be used if popliteal artery injury is suspected.[4]
According to Mustonen et al, although postoperative multidetector-row CT (MDCT) scanning of tibial plateau fractures is performed infrequently, it can in most cases reveal clinically significant information. In their study, the main indications for MDCT were assessment and follow-up of the joint articular surface and evaluation of fracture healing. Postoperative MDCT revealed additional clinically important information in 81% of patients, and 39% underwent reoperation. Orthopedic hardware caused no diagnostic problems with MDCT.[6]
Examples of tibial plateau fractures are provided in the images below:
Tibial
plateau fractures. Line drawings of Schatzker types I, II, and III
tibial plateau fractures. Type I consists of a wedge fracture of the
lateral tibial plateau, produced by low-force injuries. Type II combines
the wedge fracture of the lateral plateau with depression of the
lateral plateau. Type III fractures are classified as those with
depression of the lateral plateau but no associated wedge fracture. Tibial
plateau fractures. Line drawings of Schatzker types IV, V, and VI
tibial plateau fractures. Type IV is similar to type I fracture, except
that it involves the medial tibial plateau as opposed to the lateral
plateau. Greater force is required to produce this type of injury. Type V
fractures are termed bicondylar and demonstrate wedge fractures of both
the medial and lateral tibial plateaus. Finally, type VI fractures
consist of a type V fracture along with a fracture of the underlying
diaphysis and/or metaphysis. Tibial
plateau fractures. CT image through the tibial plateau shows a fracture
of the posterior aspect of the lateral tibial plateau, which is the
source of the lipohemarthrosis. Tibial
plateau fractures. MRI of the knee in a patient with tibial plateau
fracture and lipohemarthrosis. Three layers of effusion are demonstrated
on this proton density sequence: fat, red blood cells, and serum.
Low-signal intensity in the tibial plateau corresponds to the site of
fracture. Tibial
plateau fractures. Radiograph of the knee shows lateral plateau
splitting, a Schatzker I injury. There is no articular depression. Soft
tissue injuries (eg, to cruciate and collateral ligaments) occur in
approximately 10% of patients. In particular, medial plateau injuries
may result in fracture of the fibular head, which may injure the
peroneal nerve or may be associated with popliteal artery occlusion.
Patients may present with a knee effusion, pain, and joint stiffness.
Finally, although severe fractures often are repaired surgically, both
operatively and nonoperatively treated fractures are at risk of
developing posttraumatic osteoarthritis as a result of ligamentous
injuries with resultant instability as well as articular discongruities,
biomechanical alteration of normal compressive forces, and cartilage
damage.Preferred examination
The preferred examination consists of radiographs in multiple obliquities of the knee. Typically, these include anteroposterior (AP), cross-table lateral, patellar (sunrise), and, possibly, oblique views. Cross-table lateral and AP may be the only views possible in the trauma suite. In this setting, the cross-table lateral radiograph may be the most important to detect occult fractures. The presence of these subtle fractures may be inferred by the presence of a lipohemarthrosis on the cross-table lateral radiograph, indicating disruption of an articular surface, most often the tibia. The images below demonstrate the radiographic, computed tomography (CT), and magnetic resonance imaging (MRI) appearance of lipohemarthrosis.Tibial
plateau fractures. Cross-table lateral radiograph of the knee shows the
lipohemarthrosis within the suprapatellar bursa. The fracture itself is
not seen well. Tibial
plateau fractures. CT image through the tibial plateau shows a fracture
of the posterior aspect of the lateral tibial plateau, which is the
source of the lipohemarthrosis. Tibial plateau fractures. Axial CT image through the knee shows a layering lipohemarthrosis. Tibial
plateau fractures. MRI of the knee in a patient with tibial plateau
fracture and lipohemarthrosis. Three layers of effusion are demonstrated
on this proton density sequence: fat, red blood cells, and serum.
Low-signal intensity in the tibial plateau corresponds to the site of
fracture. CT is used by most orthopedists to further
characterize fractures of the tibial plateau and assess the depression
of the tibia and the degree of diastasis (splitting) of the fractured
parts to plan for surgical intervention. Generally, slice thickness
should be minimized (1 mm is ideal) and high milliamperage-second (mAs)
technique used.[1, 2, 3] MRI may be used as well for this determination but often is not readily available. MRI is excellent for depicting ligamentous and meniscal injuries.
Arteriography (and possibly MR angiography) may be used if popliteal artery injury is suspected.[4]
Limitations of techniques
Nondepressed tibial plateau fractures occasionally are difficult to appreciate with standard radiographs. Cross-table lateral radiographs may demonstrate a lipohemarthrosis within the joint, with layering of bone marrow fat upon blood. If lipohemarthrosis is present, an intra-articular fracture is present and must be located. In this situation, axial CT is an excellent tool for defining fracture anatomy using reconstructed images in the sagittal and coronal planes.Recent studies
Brunner et al found that CT scanning improved the interobserver and intraobserver reliability of the Schatzker, OTA/AO, and Hohl classification systems for tibial plateau fractures. The 3 systems showed moderate interobserver reliability and good and moderate intraobserver reliability when based only on findings on plain radiographs. Interobserver and intraobserver reliability improved significantly when CT was added.[5]According to Mustonen et al, although postoperative multidetector-row CT (MDCT) scanning of tibial plateau fractures is performed infrequently, it can in most cases reveal clinically significant information. In their study, the main indications for MDCT were assessment and follow-up of the joint articular surface and evaluation of fracture healing. Postoperative MDCT revealed additional clinically important information in 81% of patients, and 39% underwent reoperation. Orthopedic hardware caused no diagnostic problems with MDCT.[6]
Radiography
Many
methods have been developed to classify tibial plateau fractures. The
best known method is the Schatzker system, as depicted in the images
below:
Tibial
plateau fractures. Line drawings of Schatzker types I, II, and III
tibial plateau fractures. Type I consists of a wedge fracture of the
lateral tibial plateau, produced by low-force injuries. Type II combines
the wedge fracture of the lateral plateau with depression of the
lateral plateau. Type III fractures are classified as those with
depression of the lateral plateau but no associated wedge fracture. Tibial
plateau fractures. Line drawings of Schatzker types IV, V, and VI
tibial plateau fractures. Type IV is similar to type I fracture, except
that it involves the medial tibial plateau as opposed to the lateral
plateau. Greater force is required to produce this type of injury. Type V
fractures are termed bicondylar and demonstrate wedge fractures of both
the medial and lateral tibial plateaus. Finally, type VI fractures
consist of a type V fracture along with a fracture of the underlying
diaphysis and/or metaphysis. Type I fractures (demonstrated in
image below) are split fractures of the lateral tibial plateau, usually
in younger patients. No depression is seen at the articular surface.
Tibial
plateau fractures. Radiograph of the knee shows lateral plateau
splitting, a Schatzker I injury. There is no articular depression. Type
II fractures (shown in images below) are split fractures with
depression of the lateral articular surface and typically are seen in
older patients with osteoporosis.
 Tibial
plateau fractures. Radiograph of the knee shows a fracture through the
lateral tibial plateau with extension to the lateral tibial margin and
slight depression at the articular surface. This is a Schatzker II
injury.
Tibial
plateau fractures. Radiograph of the knee shows a fracture through the
lateral tibial plateau with extension to the lateral tibial margin and
slight depression at the articular surface. This is a Schatzker II
injury.  Tibial plateau fractures. A different patient illustrates a Schatzker II injury with subtle lateral articular depression.
Tibial plateau fractures. A different patient illustrates a Schatzker II injury with subtle lateral articular depression. 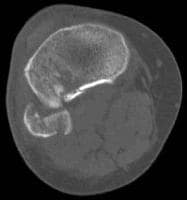 Tibial
plateau fractures. Axial CT image through the tibial shows a fracture
through the lateral tibial plateau with slight diastasis between the
fragments. This is a Schatzker II injury.
Tibial
plateau fractures. Axial CT image through the tibial shows a fracture
through the lateral tibial plateau with slight diastasis between the
fragments. This is a Schatzker II injury. 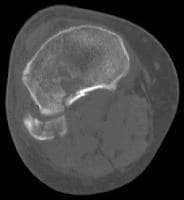 Tibial
plateau fractures. Axial CT image of the same patient as in the
previous image shows the extent of the lateral tibial plateau fracture.
In this case, it extends to the lateral tibial margin and an associated
fibular head fracture is seen. This is a Schatzker II injury. Type
III fractures (shown in image below) are characterized by depression of
the lateral tibial plateau, without splitting through the articular
surface.
Tibial
plateau fractures. Axial CT image of the same patient as in the
previous image shows the extent of the lateral tibial plateau fracture.
In this case, it extends to the lateral tibial margin and an associated
fibular head fracture is seen. This is a Schatzker II injury. Type
III fractures (shown in image below) are characterized by depression of
the lateral tibial plateau, without splitting through the articular
surface.
 Tibial
plateau fractures. Oblique radiograph of the knee demonstrates a
fracture of the lateral tibial plateau with slight depression. There is
no associated wedge component. This is a Schatzker III injury. Type IV fractures involve the medial tibial plateau and may be split fractures with or without depression.
Tibial
plateau fractures. Oblique radiograph of the knee demonstrates a
fracture of the lateral tibial plateau with slight depression. There is
no associated wedge component. This is a Schatzker III injury. Type IV fractures involve the medial tibial plateau and may be split fractures with or without depression.
Type V fractures are characterized by split fractures through both the medial and lateral tibial plateaus.
Type VI fractures (demonstrated in the images below) are the result of severe stress and result in dissociation of the tibial plateau region from the underlying diaphysis.
 Tibial
plateau fractures. Radiograph of the knee reveals fractures through
both the medial and the lateral tibial plateau along with a fibular head
fracture and a fracture through the tibial metaphysis. This is a
Schatzker VI injury.
Tibial
plateau fractures. Radiograph of the knee reveals fractures through
both the medial and the lateral tibial plateau along with a fibular head
fracture and a fracture through the tibial metaphysis. This is a
Schatzker VI injury.  Tibial plateau fractures. Radiograph of the knee shows a different Schatzker VI fracture.
Tibial plateau fractures. Radiograph of the knee shows a different Schatzker VI fracture.  Tibial
plateau fractures. Coronal reformatted CT. This image demonstrates a
bicondylar fracture of the tibial plateau along with a fracture of the
tibial diaphysis, a Schatzker VI fracture. Note the articular
incongruity.
Tibial
plateau fractures. Coronal reformatted CT. This image demonstrates a
bicondylar fracture of the tibial plateau along with a fracture of the
tibial diaphysis, a Schatzker VI fracture. Note the articular
incongruity.
Tibial
plateau fractures. Line drawings of Schatzker types I, II, and III
tibial plateau fractures. Type I consists of a wedge fracture of the
lateral tibial plateau, produced by low-force injuries. Type II combines
the wedge fracture of the lateral plateau with depression of the
lateral plateau. Type III fractures are classified as those with
depression of the lateral plateau but no associated wedge fracture. Tibial
plateau fractures. Line drawings of Schatzker types IV, V, and VI
tibial plateau fractures. Type IV is similar to type I fracture, except
that it involves the medial tibial plateau as opposed to the lateral
plateau. Greater force is required to produce this type of injury. Type V
fractures are termed bicondylar and demonstrate wedge fractures of both
the medial and lateral tibial plateaus. Finally, type VI fractures
consist of a type V fracture along with a fracture of the underlying
diaphysis and/or metaphysis. Type I fractures (demonstrated in
image below) are split fractures of the lateral tibial plateau, usually
in younger patients. No depression is seen at the articular surface.Tibial
plateau fractures. Radiograph of the knee shows lateral plateau
splitting, a Schatzker I injury. There is no articular depression. Type
II fractures (shown in images below) are split fractures with
depression of the lateral articular surface and typically are seen in
older patients with osteoporosis.Tibial
plateau fractures. Radiograph of the knee shows a fracture through the
lateral tibial plateau with extension to the lateral tibial margin and
slight depression at the articular surface. This is a Schatzker II
injury. Tibial plateau fractures. A different patient illustrates a Schatzker II injury with subtle lateral articular depression. Tibial
plateau fractures. Axial CT image through the tibial shows a fracture
through the lateral tibial plateau with slight diastasis between the
fragments. This is a Schatzker II injury. Tibial
plateau fractures. Axial CT image of the same patient as in the
previous image shows the extent of the lateral tibial plateau fracture.
In this case, it extends to the lateral tibial margin and an associated
fibular head fracture is seen. This is a Schatzker II injury. Type
III fractures (shown in image below) are characterized by depression of
the lateral tibial plateau, without splitting through the articular
surface.Tibial
plateau fractures. Oblique radiograph of the knee demonstrates a
fracture of the lateral tibial plateau with slight depression. There is
no associated wedge component. This is a Schatzker III injury. Type IV fractures involve the medial tibial plateau and may be split fractures with or without depression. Type V fractures are characterized by split fractures through both the medial and lateral tibial plateaus.
Type VI fractures (demonstrated in the images below) are the result of severe stress and result in dissociation of the tibial plateau region from the underlying diaphysis.
Tibial
plateau fractures. Radiograph of the knee reveals fractures through
both the medial and the lateral tibial plateau along with a fibular head
fracture and a fracture through the tibial metaphysis. This is a
Schatzker VI injury. Tibial plateau fractures. Radiograph of the knee shows a different Schatzker VI fracture. Tibial
plateau fractures. Coronal reformatted CT. This image demonstrates a
bicondylar fracture of the tibial plateau along with a fracture of the
tibial diaphysis, a Schatzker VI fracture. Note the articular
incongruity. Degree of confidence
Most fractures of the tibial plateau are diagnosed readily by conventional radiography.False positives/negatives
A false-negative radiograph may be encountered on the rare occasions in which a fracture is present but only a lipohemarthrosis is visualized. In these patients, CT or MRI is required to visualize the fracture.Computed Tomography
In
most patients, CT scanning mimics the findings of conventional
radiography. With reconstruction of the axial images into coronal and
sagittal planes, precise localization of surgical landmarks, as well all
fracture fragments, is obtained. CT is critical in formulating a
surgical plan for Schatzker type IV, V, and VI fractures.[7]
Although, as previously mentioned, most fractures of the tibial plateau are diagnosed readily by conventional radiography, CT often is used to confirm the anatomic relationship of fracture fragments with more complex fractures. This is especially true at the articular surface of the tibia, where precise 3-dimensional anatomy is critical to the success of surgical repair. Less comminuted and depressed fractures may not require imaging by CT.
The value of CT is in the speed and availability of the technique. In addition, most patients with extensive injuries also undergo CT of other portions of the body in the trauma setting. With current scanners, image thickness of 1 mm or less is possible, which generally yields unequivocal depiction of fracture patterns. However, for a full depiction of soft tissue injury, such as ligaments and menisci, MRI is superior.
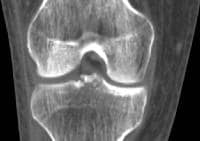 Tibial
plateau fractures. Coronal reformatted CT. Initial narrow collimation
axial CT data can be reconstructed into sagittal and coronal planes.
This technique is useful to evaluate for fracture lines parallel to the
axial imaging plane, degree of articular depression, and degree of
diastasis between major fracture fragments. The best reconstructions are
made when the initial data set consists of axial images of less than 2
mm thickness. In this particular case, an axial data set of 1 mm images
was reconstructed into this coronal image demonstrating fractures of the
tibial spines. Tibial
plateau fractures. Coronal reformatted CT. This image demonstrates a
bicondylar fracture of the tibial plateau along with a fracture of the
tibial diaphysis, a Schatzker VI fracture. Note the articular
incongruity.
Tibial
plateau fractures. Coronal reformatted CT. Initial narrow collimation
axial CT data can be reconstructed into sagittal and coronal planes.
This technique is useful to evaluate for fracture lines parallel to the
axial imaging plane, degree of articular depression, and degree of
diastasis between major fracture fragments. The best reconstructions are
made when the initial data set consists of axial images of less than 2
mm thickness. In this particular case, an axial data set of 1 mm images
was reconstructed into this coronal image demonstrating fractures of the
tibial spines. Tibial
plateau fractures. Coronal reformatted CT. This image demonstrates a
bicondylar fracture of the tibial plateau along with a fracture of the
tibial diaphysis, a Schatzker VI fracture. Note the articular
incongruity.
Although, as previously mentioned, most fractures of the tibial plateau are diagnosed readily by conventional radiography, CT often is used to confirm the anatomic relationship of fracture fragments with more complex fractures. This is especially true at the articular surface of the tibia, where precise 3-dimensional anatomy is critical to the success of surgical repair. Less comminuted and depressed fractures may not require imaging by CT.
The value of CT is in the speed and availability of the technique. In addition, most patients with extensive injuries also undergo CT of other portions of the body in the trauma setting. With current scanners, image thickness of 1 mm or less is possible, which generally yields unequivocal depiction of fracture patterns. However, for a full depiction of soft tissue injury, such as ligaments and menisci, MRI is superior.
False positives/negatives
CT generally is able to depict all fractures. False-negative errors can occur when only axial imaging is used. If a fracture predominates in the axial plane, it may be overlooked by CT. However, in most instances, sagittal and coronal reconstructions of axial data, as shown in the images below, are used to avoid this problem. By reconstructing the initial data set into different planes, additional information such as articular depression and diastasis may be obtained easily. False positives are not common with CT.Tibial
plateau fractures. Coronal reformatted CT. Initial narrow collimation
axial CT data can be reconstructed into sagittal and coronal planes.
This technique is useful to evaluate for fracture lines parallel to the
axial imaging plane, degree of articular depression, and degree of
diastasis between major fracture fragments. The best reconstructions are
made when the initial data set consists of axial images of less than 2
mm thickness. In this particular case, an axial data set of 1 mm images
was reconstructed into this coronal image demonstrating fractures of the
tibial spines. Tibial
plateau fractures. Coronal reformatted CT. This image demonstrates a
bicondylar fracture of the tibial plateau along with a fracture of the
tibial diaphysis, a Schatzker VI fracture. Note the articular
incongruity. Magnetic Resonance Imaging
The
role of MRI in the acute management of tibial plateau fractures is
under investigation. A study by Kode et al investigated the usefulness
of CT and MRI in visualizing fracture patterns.[8] MRI
was superior to CT unless the fracture was extremely comminuted.
Meniscal injuries, as well as injuries to the collateral and cruciate
ligaments, are depicted better with MRI than with CT. (See the image
below.)[9]
Tibial
plateau fractures. MRI of the knee in a patient with tibial plateau
fracture and lipohemarthrosis. Three layers of effusion are demonstrated
on this proton density sequence: fat, red blood cells, and serum.
Low-signal intensity in the tibial plateau corresponds to the site of
fracture.
Tibial
plateau fractures. MRI of the knee in a patient with tibial plateau
fracture and lipohemarthrosis. Three layers of effusion are demonstrated
on this proton density sequence: fat, red blood cells, and serum.
Low-signal intensity in the tibial plateau corresponds to the site of
fracture. Degree of confidence
MRI is very sensitive to the presence of osseous injury. Injuries to osseous structures manifest as areas of edema within bone marrow. However, fractures through the cortex are less well depicted, as cortical bone appears as an area of low signal (generally black) on MRI sequences. Thus, fractures through cortical bone can be difficult to depict with MRI. Complex and comminuted fractures with multiple cortical fragments are exceedingly difficult to analyze with MRI.False positives/negatives
False negatives with MRI are uncommon. MRI is used routinely for the detection of occult fracture because of its superior depiction of bone marrow edema, a direct indicator of osseous injury. False-negative information may result when MRI data is analyzed for the presence of cortical fractures. False-negative and false-positive errors may occur if the incorrect MRI sequences are chosen. In general, a fluid sensitive sequence, such as short tau inversion recovery, rather than a simple T2-weighted sequence, is best to detect bone marrow edema.Nuclear Imaging
Nuclear
medicine studies are not used in the diagnosis of tibial plateau
fractures, unless a stress-type fracture is suspected or there is
concern that osteomyelitis exists.
Angiography
Type IV fractures involving the medial tibial plateau raise concern that the popliteal artery has been injured. These arterial injuries can be clinically silent or present with decreased peripheral pulses.If clinical concern exists that a popliteal artery injury has occurred with any fracture type, obtain an arteriogram (or possibly an MR angiogram). Surgical manipulation of the tissues surrounding an injured popliteal artery can result in thrombosis, with dire consequences unless the thrombosis is addressed immediately.
However, angiography is not used for the primary detection of tibial plateau fractures
No comments:
Post a Comment